EndoscopyHome
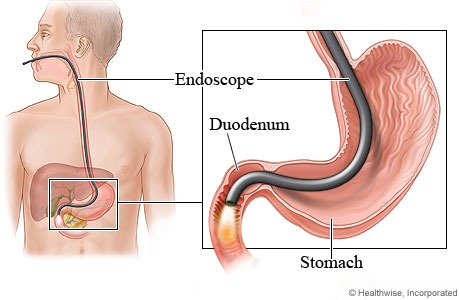
Endoscopy is the procedure of examining the inside of human body for some medical reasons by using a rigid and flexible telescope known as endoscope.
It is minimally invasive diagnostic medical procedure used to examine the internal surfaces of an organ or tissue.
When other diagnosis devices are considered inappropriate like MRI, CT Scan and X- Ray, it is often used to confirm the degree of problems where certain conditions may have caused.
With the help of this, the visualization of ovaries, uterus and tubes etc are possible without having a big cut and helps to operate inside at the same sitting. Procedure is very helpful to examine the following parts of body:
- The Uterus
- The Fallopian Tube
- Ovaries
- Endometriosis
Further ,In our clinic we always perform Laparoscopy and Hysteroscopy and required procedure in the same sitting. Like repair of the tubes, correction of endometriosis, ovarian drilling for Polycystic Ovarian Disease.
In Hysteroscopy ,the inside of the uterine lining is seen . With this technique we perform various procedures like Tubal cannulation ( for blocked fallopian tubes), removal of polyps, Septum resection etc. The main purpose of doing this procedure is to make the uterine bed good, so that embryo should implant
In Laparoscopy and Hysteroscopy ,the female partner is asked to come overnight fasting. It requires general anesthesia and may require one day hospital stay
Hysteroscopy: Hysteroscopy is a minor surgical procedure that involves placing a lighted telescopic instrument (hysteroscope) through the neck of the womb (uterine cervix) and visualizing any abnormalities within the wall of the uterine cavity.
- Diagnostic
- Uterine Septum Resection
- Lateral Metroplasty
- Adhesiolysis [Asherman’s Syndrome]
- Polypectomy
- TCRE
- Tubal Cannulation
- Submucous Myoma Resection
- Foreign Body Removal
Operative Laparoscopy:
- Diagnostic
- Ovarian Cyst:
1. Simple Cyst
2. Chocolate Cyst
3. Para ovarian Cyst
4. Dermoid Cyst
- Endometrail Fulgration
- Adhesiolysis
- Fimbrioplasty
- Poly Cystic Ovarian Drilling
- Single Puncture Tubal Ligation [Lap TL]
- Myomectomy
- Laparoscopic Management of Ectopic Pregnancy
- Laparoscopic Management of Ovarian Torsion
- Total Laparoscopic Hysterectomy
- Tubal recanalisation
- Uterine Unification Surgery
Chromotubation (Dye Test for tubal patency): It is a procedure usually done during an infertility work-up. During laparoscopy, a colored dye will be introduced into the uterine cavity being injected through the cervical canal during the procedure and then observed as it comes out of the ends of the tubes into the peritoneal (abdominal) cavity to check tubal patency.
Tubal Surgery for damaged fallopian tube(s):
- Adhesiolysis (freeing the tubes): If the tubes and ovaries are covered in fine adhesions from previous pelvic inflammation, eggs in the ovaries have no access to the open end of the fallopian tubes and a pregnancy is not possible. The laparoscopic adhesiolysis procedure performed to surgically remove all adhesions (salpingo-oophorolysis).
- Tuboplasty (Unblocking the fallopian tubes): The blocked outer end of the tube is opened at laparoscopy. These procedures are called Salpingostomy or Neosalpinostomy (creation of new opening in the tube).
- Salpingectomy (removal of tube(s) if badly damaged): Collection of fluid in the fallopian tube (hydrosalpinx) damages the tube; this will put the women at risk of ectopic pregnancy and also decreases the IVF success rates. This is due to the back flow of fluid from hydrosalpinx may be toxic to the embryo’s transferred and it will prevent from implantation. Hence, it will be better to remove the fallopian tube to optimize IVF success rate and prevent ectopic pregnancies.
Ovarian Cystectomy & Other Ovarian Procedures:
- Ovarian drilling for treatment of PCOS: PCOS can be treated with drugs or surgery. The advantage of having surgery is that it does not increase the risk of multiple births. In this procedure (ovarian drilling), a heated needle (electro diathermy) is used to destroy some of the extra follicles (the sacs in which eggs develop) which are producing an excess of male hormones.
- Surgical Treatment to endometriosis: Laparoscopy is the most common (gold standard) procedure used to diagnose and to remove mild to moderate endometriosis. If at laparoscopy deposits of endometriosis in the ovaries and pelvic ligaments are found, these may be destroyed at the time with electro diathermy. If the endometriosis is more extensive, further surgery is offered where the endometriotic tissue is removed by Cautery / excision of endometriosis.
- Endometriotic ovarian cyst(s) removal or aspiration: A common complication of endometriosis is the development of a cyst on an ovary. This blood-filled growth is called an ovarian endometrioma or an endometriotic or chocolate cyst.
- Other benign ovarian cyst(s) removal: Ovarian cysts are fluid-filled sacs in the ovaries. They are very common in women, especially during the childbearing years. Ovarian cysts usually cause no symptoms. Most ovarian cysts will disappear without any intervention. However, they can persist, increase in size and can create a dull ache or a sharp pain if one twists or ruptures. Laparoscopic treatment includes draining (aspiration) , cutting out part of it, or removing it completely (cystectomy).
- Mobilization of ovaries & fallopian tubes from bowel and pelvic adhesions
- Myomectomy (Surgical removal of fibroids through laparoscopy)
OTHER PROCEDURES:
Myomectomy (open):
Myomectomy is surgery to remove the fibroid, preserving as much of the normal uterine muscle as possible. If the fibroids are mostly within the wall of the uterus, the surgery is usually done by laparotomy, that is, performing an open abdominal incision and cutting into the uterus from the external surface. Most of the gynecologists can perform this surgical procedure. Risks to the procedure are minimal but may include bleeding and damage to the normal uterine muscle. Many patients will have pelvic scar tissue forming as a result of the open abdominal incision and the uterine incisions. Most patients that have a myomectomy will need to have a Cesarean section with any subsequent pregnancy.
Tubal recanalization (Sterilization reversal):
Before considering a reversal of sterilization, it would make sense to ensure that partner’s semen analysis shows a normal sperm count. There would be little point in undergoing major surgery to subsequently find that partner’s sperm count is zero.
Sterilization can be reversed where the procedure was achieved by: cutting and then tying the fallopian tubes by blocking the tubes by placing a small plastic clip or ring across them.
The reversal will depend upon the site of the sterilization on each tube, and, in the case of cutting and tying the tubes, how much healthy tube remains.
If the sterilisation has been performed using electro diathermy, usually the entire tube will have been destroyed and reversal is not possible. If the sterilisation site is close to the junction of the tube to the uterus, and not much tube has been removed or destroyed, the successful delivery rate after reversal of sterilisation should be above 70%. Microsurgical techniques are normally used to rejoin two sections of undamaged tube, enabling it to function normally again. The risk of this procedure is tubal pregnancy (ectopic). In present era, IVF is an better alternative to the reversal of sterilization.